Huge progress has been made in recent years in the battle to rid the world of neglected tropical diseases (NTDs) – a group of 20 diseases that debilitate, disfigure and kill. Forty-three countries have eliminated at least one NTD, 600 million people no longer require treatment, and cases of some of the diseases that have plagued humanity for centuries, such as sleeping sickness and Guinea worm disease, are at an all-time low. Elimination of NTDs as a public health problem seems within reach.
Yet, more work still needs to be done. 1.5 billion people are currently impacted by NTDs, and health systems remain inadequate in many countries. Amidst the burden of the Covid-19 pandemic on healthcare services and supply chains, and the uncertain future of external financing, innovative tools and techniques to expedite elimination efforts have never been more vital.
As part of the ARISE project, which is funded by the Children’s Investment Fund Foundation, our teams have been applying new ‘Precision-mapping’ protocols to enhance efforts to combat the NTD, schistosomiasis. This disease is caused by an infection with parasitic worms that live in certain types of snails. Eggs laid by the worms can cause anaemia and stunting in childhood, and if left untreated can lead to liver fibrosis, kidney failure or bladder cancer.
Schistosomiasis is a localised disease, mainly occurring near freshwater habitats where the infected snails live. Treatment for the infection is safe and simple – one tablet once a year can reduce morbidity associated with infection. Yet, in a world of limited resources it is vital that governments have accurate data on where the disease is prevalent to allow for targeted control efforts as well as to combat ongoing transmission.
Precision mapping enables this by using ‘mapping’ exercises and data to deduce exactly where transmission is happening. Unlike earlier mapping approaches, precision mapping conducts sampling at a much smaller geographical resolution, more reflective of the nature of schistosomiasis transmission.
Working with governments in Uganda, Kenya, and Tanzania, through the use of precision mapping, ARISE is supporting Ministries of Health collect improved information on exactly which areas of the country still require treatment. The updated maps then guide the governments’ next steps around NTD control and focus treatment and prevention activities on areas most in need.
These include Mass Drug Administration (MDA) campaigns which can be more targeted to affected regions, avoiding over-treatment and undertreatment, and making best use of the limited stock of donated medicines. Our recent precision mapping exercise was conducted in Uganda, where previous treatment campaigns, which had been regularly running since the 1950s, and were costing the government and international donors hundreds of thousands of pounds per year.2.
Our exercise identified the levels of endemicity in local villages, so that the government would have a better idea of whether to continue with blanket MDAs of all communities in these regions. ARISE organised 13 teams of technicians, auxiliary workers, researchers and disease experts to visit 800 villages. The teams worked tirelessly, covering two villages per day, and taking over 13 days in total. To identify cases of schistosomiasis, local children’s stool and urine samples needed to be examined for the presence of worm eggs, so it was vital the teams gained the trust of the children and their families to support the activity. By the end of the exercise over 41,000 children had provided samples for testing.

Make-shift laboratories were set up in the local area to ensure samples were analysed quickly and effectively. These were mostly under shaded trees, but the teams were open to the elements – with one exercise being halted due to a snake making a home in the new lab!
Special sieves, medical cellophane, urine filtration kits, microscopes and unique helminth test kits were used to gather the data. This was then recorded in KoBo Collect, an open-source data app, uploaded on the team’s mobile phones. The easy-to-use interface avoided cumbersome paper data collection, reporting and collation, and has in-built data validation to minimise data entry errors.
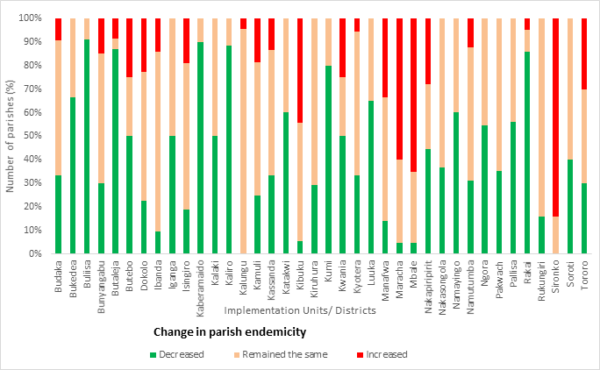
The final results painted an unexpected story of schistosomiasis endemicity in Uganda, with some areas that were being regularly treated showing low or no infection levels, and other areas requiring intensified treatment efforts. The information is enabling the Ministry of Health to home-in on local risk factors and put in place stronger preventative measures. This might include additional rounds of MDA or the distribution of targeted health education materials. Yet, for most of the regions the research showed a reduction in schistosomiasis which has guided a reallocation of resources and even the halting of treatment areas where it is no longer warranted.
The use of precision mapping as an NTD control and elimination tool has enabled the scaling down of future schistosomiasis MDAs in Uganda, which will ultimately save health worker effort and provide savings for the government, as less drugs would need to be purchased. Not only will this mean resources can be reallocated to other health services, but also support acceleration of Uganda’s NTD elimination goals.
Thank you to the Ministry of Health in Uganda for their collaboration and leadership in the SCH precision mapping.